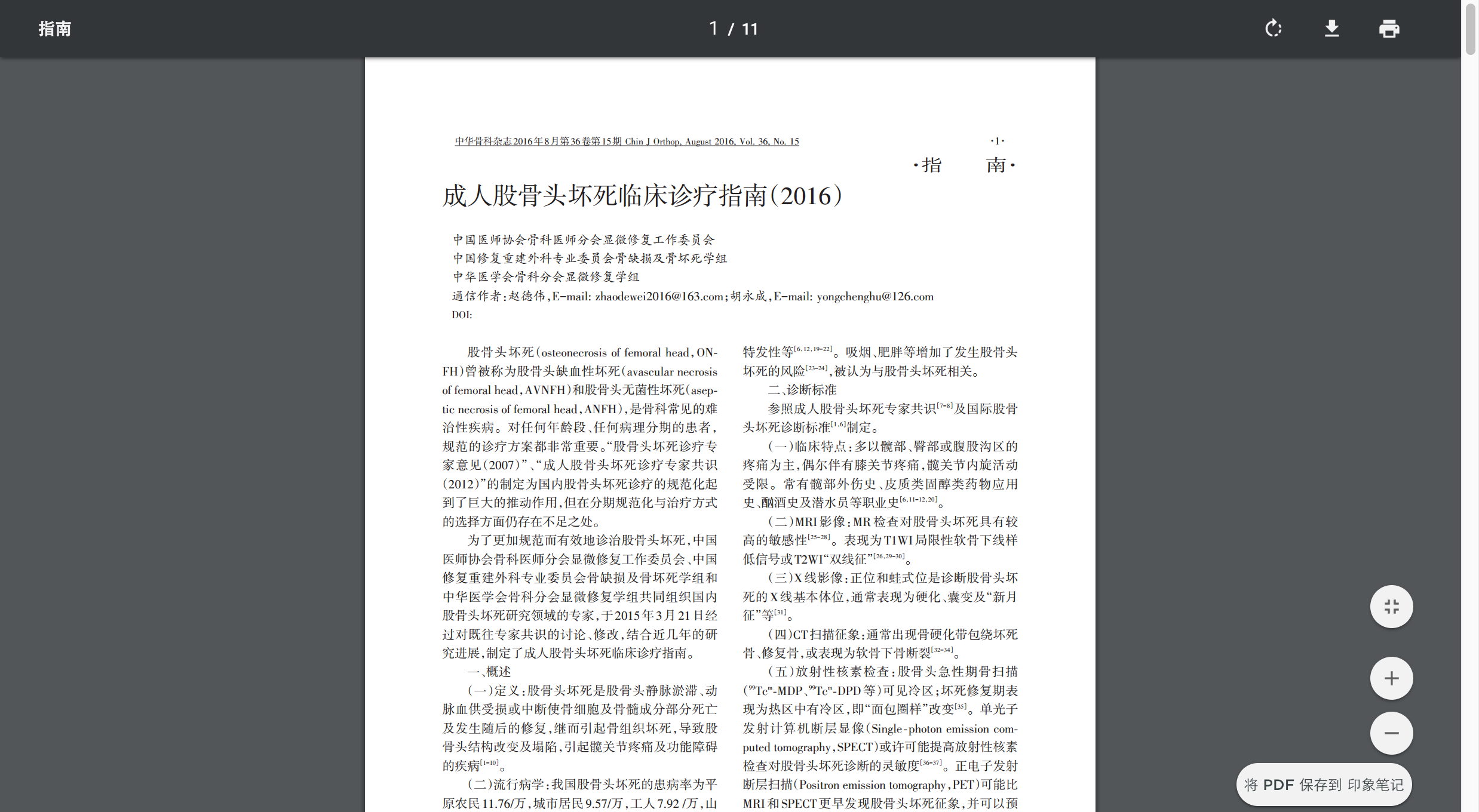
骨干组配式假体的研究现状
2016年11月19日 胡永成 伦登兴 赵立明
Stryker system(史塞克公司)是第一家骨干肿瘤假体制作公司,主要包括2代产品[2,6,11]。第一代产品(图1)远、近端柄的链接方式是锥度链接,主要缺陷是:术中需要过度牵拉才能使假体复位,神经相关并发症较多;且锥度链接并不稳定,容易出现假体脱位或骨折等并发症。因此,第二产品由锥度链接改为搭接型链接,可通过2枚螺钉固定两端假体柄,操作相对简单,不会因过度牵拉导致神经损伤;但应力集中或应力转移等使假体松动仍不能解决。Stryker system的两代产品均由远端、近端柄构成,没有独立的假体重建组件或假体延长组件,重建缺损长度有限。图1 Stryker system 骨干组配式假体OsteoBridge IDSF spacer system[12,13,19]有四部分组成:远端柄、近端柄及2个半圆桥形假体重建部件(upper and lower half-shell)。术中可根据骨缺损的长度,选择不同尺寸的一个或多个半圆桥型假体重建骨缺损。重建骨缺损长度分为4-17cm。远、近端假体柄与残留骨之间可通过2枚螺钉固定,半圆桥型重建部件可通过8枚螺钉固定,即桥型链接,但部分假体也通过滑行链接。优点是2个半圆桥型之间可以填充自体骨或异体骨,利于骨长入;但假体断裂、松动柄并未减少。图2 OsteoBridge IDSF spacer system骨干组配式假体Depuy synthes LPS system有3部分组成,包括远端柄、近端柄及假体重建部件。柄与重建组件之间通过单纯锥度链接固定。操作相对简单。但存在更多缺陷:1、适应证部位较小,仅为股骨干缺损;2、适应骨缺损尺度有限,骨水泥型骨干假体长度100-125mm,柄直径10-17ml;多孔非骨水泥假体长度100-125mm,柄直径11.5-18.5cm;3、目前文献报道的临床应用有限,单纯锥度链接是否稳定仍需进一步验证。图3 Depuy synthes LPS system骨干组配式假体Stanmore system[7,9,13]和K-MAX system[20]主要设计并制作定制型骨干假体,尤其是Stanmore system应用非常广泛,且文献报道较多。但假体相关并发症较多;且假体制作时间较长,可能延误治疗时间;尤其是对于骨干转移瘤伴病理性骨折患者,生命期限较短。骨干组配式假体应该是该类患者最好的重建方法。根据以上各种假体的优、缺点,我们设计一种新的骨干组配式假体(HU intercalary diaphyeal modular system-I, HIDMS),主要包括四部分:远端柄和/或外侧钢板、假体重建段、延长接头及近端柄和/或内外侧钢板(图4a)。根据肿瘤不同部位,选择不同假体类型(图4b-d)。当肿瘤位于A区或C区时,单纯骨干假体不稳定,需增加额外钢板。其中假体柄与假体重建段通过搭接方式固定,延长接头与假体重建段和假体柄通过锥度链接固定。避免传统锥度链接过度牵拉引起神经损伤,使操作简单;又能充分利用搭接型链接的稳定性,避免假体松动、断裂。从骨水泥固定向生物型固定的改变,可以明显提高人工假体的使用寿命;随着3D打印技术的发展使假体由组配式向“个性化”的方向改变,实现了不同患者的个体化治疗目标;随着人工假体置换手术从老年人和转移瘤患者向年轻人和原发性肿瘤的方向改变,促进了假体长期稳定性影响因素的研究。我们相信:随着假体固定方式随着3D打印技术在肿瘤假体制作及假体表面处理中的应用,HIDMS将会为更加骨肿瘤医师提供方便,提高治疗效果。图4 HIDMS骨干组配式假体参考文献1. Clain A. Secondary malignant disease of bone. Br J Cancer 1965;19:15-29.2. Chin HC, Frassica FJ, Hein TJ, Shives TC, Pritchard DJ, Sim FH, Chao EY. Metastatic diaphyseal fractures of the shaft of the humerus. The structural strength evaluation of a new method of treatment with a segmental defect prosthesis. Clin Orthop Relat Res. 1989;(248):231-9.3. Guzik G. Results of the treatment of bone metastases with modular prosthetic replacement--analysis of 67 patients. J Orthop Surg Res. 2016 Feb 5;11:20. doi: 10.1186/s13018-016-0353-6..4. Mankin HJ, Gebhardt MC, Jennings LC, Springfield DS, Tomford WW. Long-term results of allograft replacement in the management of bone tumors. Clin Orthop Relat Res, 1996, 324: 86–97.5. Sakellariou VI, Mavrogenis AF, Papagelopoulos PJ. Limb salvage surgery using the intramedullary diaphyseal segmental defect fixation system. J Long Term Eff Med Implants. 2008;18(1):59-67.6. Damron TA, Sim FH, Shives TC, An KN, Rock MG, Pritchard DJ. Intercalary spacers in the treatment of segmentally destructive diaphyseal humeral lesions in disseminated malignancies. Clin Orthop Relat Res. 1996 ; (324):233-43.7. Abudu A, Carter SR, Grimer RJ. The outcome and functional results of diaphyseal endoprostheses after tumour excision. J Bone Joint Surg Br. 1996;78: 652-7.8. Henry JC, Damron TA, Weiner MM, Higgins ME, Werner FW, Sim FH. Biomechanical analysis of humeral diaphyseal segmental defect fixation. Clin Orthop Relat Res. 2002; 396:231-9.9. Aldlyami E, Abudu A, Grimer RJ, Carter SR, Tillman RM. Endoprosthetic replacement of diaphyseal bone defects. Long-term results. Int Orthop. 2005;29:25-9.10. Ahlmann ER, Menendez LR. Intercalary endoprosthetic reconstruction for diaphyseal bone tumours. J Bone Joint Surg Br. 2006;88:1487-91.11. Damron TA, Leerapun T, Hugate RR, Shives TC, Sim FH. Does the second-generation intercalary humeral spacer improve on the first? Clin Orthop Relat Res. 2008;466:1309-17.12. Mavrogenis AF, Sakellariou VI, Tsibidakis H, Papagelopoulos PJ. Adamantinoma of the tibia treated with a new intramedullary diaphyseal segmental defect implant. J Int Med Res. 2009;37:1238-45.13. Hanna SA, Sewell MD, Aston WJ, Pollock RC, Skinner JA, Cannon SR, Briggs TW. Femoral diaphyseal endoprosthetic reconstruction after segmental resection of primary bone tumours. J Bone Joint Surg Br. 2010;92:867-74.14. Sewell MD, Hanna SA, McGrath A, Aston WJ, Blunn GW, Pollock RC, Skinner JA, Cannon SR, Briggs TW. Intercalary diaphyseal endoprosthetic reconstruction for malignant tibial bone tumours. J Bone Joint Surg Br. 2011;93:1111-7.15. Ruggieri P, Mavrogenis AF, Bianchi G, Sakellariou VI, Mercuri M, Papagelopoulos PJ. Outcome of the intramedullary diaphyseal segmental defect fixation system for bone tumors. J Surg Oncol. 2011;104: 83-90.16. Hamada K, Naka N, Omori S, Outani H, Oshima K, Joyama S, Araki N, Yoshikawa H. Intercalary endoprosthesis for salvage of failed intraoperative extracorporeal autogeneous irradiated bone grafting (IORBG) reconstruction. J Surg Case Rep. 2014;2014(3). pii: rju014.17. Hu YC. Surgical technique for reconstruction of diaphyseal defect with endoprosthesis following intercalary resection in femoral shaft. Orthop Surg. 2014;6:329-31.18. Zhao SC, Zhang CQ, Zhang CL. Custom-made intercalary endoprosthetic reconstruction for a parosteal osteosarcoma of the femoral diaphysis: A case report. Oncol Lett. 2015;10:3279-3285.19. Benevenia J, Kirchner R, Patterson F, Beebe K, Wirtz DC, Rivero S, Palma M, Friedrich MJ. Outcomes of a Modular Intercalary Endoprosthesis as Treatment for Segmental Defects of the Femur, Tibia, and Humerus. Clin Orthop Relat Res. 2016;474:539-48.20. Hamada K, Naka N, Tamiya H, et al. Intercalary endoprosthetic reconstruction for impending pathological fractures in patients with femoral diaphyseal bone metastases[J]. European Journal of Orthopaedic Surgery & Traumatology, 2009, 19(8):547-551.胡永成 教授